Previously I provided some feedback from a Biggest Loser contestant along with my personal comments on what they told me. At the end I opined that, like most in this industry I find the show infuriating and appalling doing far more harm than good, especially for it’s target population. So today I want to present a 6-part series on training the obese beginner for both trainers and trainees.
Table of Contents
2020 Addendum: A Note on Terminology
I originally wrote this piece many years ago and, well, the world has changed. In modern times it’s becoming more accepted to refer to individuals with obesity or individuals with excess weight rather than as being obese or overweight. This seems like a semantic nitpick and, to me, it kind of is. Ok, boomer.
But the purpose of the change is primarily to shift focus from obesity defining who the individual is to it being something that the individual is I guess “dealing” with would be the right way to describe it. Specifically many now consider obesity to be a preventable, repeatable but relapsing disease.
It represents a complex set of physiological, neurological, behavioral and environmental issues and the whole idea of it being “a moral failing” or due to “sloth and gluttony” has been long abandoned. Or rather it needs to be in those places where it still exists.
The change in terminology is also meant to cause a shift in how people think about it.
Research has identified what are called fixed and growth mindsets. A fixed mindset is when you think of some aspect of yourself as being immutable. Growth mindsets allow for the improvement in some aspect of yourself. The idea that someone “is obese” can lead to a fixed mindset. It’s what you are and can’t be changed and this is not a good attitude to take into behavior change.
In contrast, conceptualizing obesity as a condition or disease that can be changed or addressed allows for a growth mindset. And this is a far better mental attitude to carry into attempts on behavior change.
It’s no different than someone thinking that they “are bad at math” which isa fixed mindset and unlikely to make them attempt to improve it. A growth mindset is much more likely to lead the person to work towards improvement and be more likely to achieve it.
Now, I acknowledge all of this, that the terminology “beginner with obesity” is more appropriate than “obese beginner”. At the same time, I’m not going to rewrite the entire 6-part series to change my terminology since it would be too exhausting. Just accept that any time I use the phrase “obese beginner” what I mean is a “beginner with obesity”.
Also, I am aware that some people think the term “obese” should be eliminated from the lexicon due to being offenssve. This is due to the amount of negative connotations it has come to be associated with and I understand that on one level. And this one I don’t buy into because I don’t believe in word or thought policing by and large. Please take that to Tumblr. I have used and will always use obese in a clinically defined term (BMI or bodyfat percentage) with no negative connotations associated with it. Anything people read into the term beyond that is their own problem, not mine.
And with that said….
Training the Obese Beginner: Introduction
Now this is going to be a long series, it came out to 6 parts when all was said and done. Today I’m just going to focus on some underlying physiology, some metabolic issues/defects that can occur in the obese. Please note that I am making no attempt to be comprehensive, that would be an entire book.
Today, I actually really want to focus only on a comment I once made
Here in Part 1, I want to focus mainly on some of the underlying physiology that occurs in the obese (and make no mistake, what I want to cover won’t be anywhere close to comprehensive; I’ll focus on issues relevant to fat loss); in Part 2-6 I’ll to look at some practical issues that I find many forget when they give advice and/or train the obese hands-on.
Today, what I actually want to do is expand on a comment I made in Fasted Cardio and Fat Loss – Q&A which was this
At the other extreme, that is in the very obese (here I’m talking about perhaps 35%+ body fat for men and 40%+ for women), the reverse problem is present. There are tons of fatty acids floating around in the bloodstream, but for a variety of reasons, oxidation has become impaired. To fully discuss this issue (along with approaches of fixing it) would require a full article series.
Well this is that article series.
What Defines an Obese Beginner?
By extremely obese here, I’m primarily using body fat percentage as the determinant. A male at 30-35%+ body fat and a female at 40%+ are in that category. It’s possible to see even higher number. In the most extremes of obesity, a BF% of 50-60% is not unheard of. Yes, this means that half or more of the person’s total weight is made up of body fat.
I won’t mess around with BMI (for discussion of this see Measuring Body Composition Part 1) though it tends to be pretty accurate in this group. That is, while they exist (usually heavier strength/power athletes taking steroids), you don’t see a lot of people at 300+ lbs body weight who aren’t carrying a lot of fat.
In general, BMI will track with body fatness, at least in a NON-ATHLETIC population.
I’d also note that it is possible for relatively lighter individuals to carry relatively more body fat (this called being skinny fat). Much of what I’m going to discuss in terms of underlying physiological “defects” will apply to that group. But for individuals who are carrying both extra weight AND fat, there are issues (mainly issues of programming) that are critical to take into account that I’ll cover later in the series.
It should be fairly obvious that by “beginner” I am referring to training or exercise level. A beginner is someone who is not currently on any type of formalized exercise program. Even in cases where someone was very active when they were younger, they should consider themselves a beginner when they return to exercise.
Let Me Be Abundantly Clear About the Word “Defect”
As one final pedantic note, so nobody takes me the wrong way, I used the term “defect” above and will continue to use that throughout the article but I want to make it absolutely clear that I’m using it in its literal sense (just as I am using “obese” in its literal, clinical sense).
That is, many physiological systems become impaired in obesity. Whether or not they are a cause or consequence of obesity is sometimes more difficult to determine. The point is that the system is impaired. That is they are defective relative to what is considered “normal” physiology (normal being another loaded word).
But I am NOT using this to try to suggest any sort of negative fashion as if obesity is some sort of defective condition. Or that the person in question is defective.
That is, the word “defect” tends to have very negative connotations (in the same way that the literal meaning of “abnormal” and the connotations that it carries are different) and I am absolutely NOT using the term in that sense. Are we clear? I’m using the term literally here, not connotatively. And that is too a word.
The Metabolic Syndrome: Part 1
If there is a singular metabolic issue (and it’s really a cluster of issues) that tends to go hand in hand with obesity, it’s what used to be called Syndrome X and is now called The Metabolic Syndrome. I’d note that while obesity tends to be one of the largest predisposing factors to development, it’s neither a guarantee nor a requirement for this to occur.
That is, there is a proportion of people who despite being obese are metabolically “normal” or “healthy” (this is called metabolically healthy obesity). This isn’t a majority, from memory it’s maybe 25% of the obese population. And there is a lot of debate over it. It seems, primarily to occur when people are obese but still active as that activity alone can offset some of the physiological problems that usually occur when someone becomes obese.
In a similar vein, it is possible to have elements of the Metabolic Syndrome such as insulin resistance and not be overweight or obese. It’s not common but it can occur. My point being that being obese is not a guarantee of developing Metabolic Syndrome although it’s extremely likely. And being skinny/lean is not a guarantee of not developing it although it’s far less common (and generally genetic).
On average, obesity tends to drastically increase the risk of developing the Metabolic Syndrome.
Now, the metabolic syndrome, as noted, is actually a cluster of different things including issues with poorly regulated blood lipid levels, high blood pressure, inflammation and a ton of other things. I’m not going to talk much about those in this series. Instead, what I want to focus on is insulin resistance.
Insulin Resistance
Now, insulin resistance, in rather simple terms, refers to a situation where various tissues in the body including skeletal muscle, liver and fat cells no longer respond appropriately to the signal sent by the hormone insulin. This has a number of consequences not the least of which is that blood sugar levels tend to become poorly regulated just as it does in diabetes.
There is not only typically an increase in fasting blood sugar levels (which is actually diagnostic for the syndrome/pre diabetes) but some strange things can occur in response to the ingestion of carbohydrates. Usually there is an overproduction of insulin in response to their consumption which can drive blood sugar too low and cause reactive hypoglycemia and/or hunger.
As well, because the liver is no longer responding appropriately to the signal sent by insulin, other bad things happen that I’m not going to detail here. The issue of insulin resistance is very involved and I’m going to skirt some details.
However, of some importance, is the fact that, when whole body insulin resistance develops, fat cells become resistant to the effects of insulin. This has a couple of consequences one of which is that insulin no longer inhibits fatty acid release which is part of what I was alluding to in the section I quoted myself on above.
Basically.
The Metabolic Syndrome: Part 2
That is, under normal conditions, in response to an increase in insulin levels (due to carbohydrate or protein consumption), the body will reduce fatty acid levels. But in the obese, this pathway is inhibited due to the development of insulin resistance.
This is also part of why drugs that cause insulin resistance such as growth hormone, clenbuterol or ephedrine, often improve fat loss. They prevent insulin from inhibiting fat release which makes it easier to mobilize the fat so it can be burned off.
But insulin resistance at the fat cell is part of why there tend to be lots of fatty acids floating around in the bloodstream all the time in folks with metabolic syndrome.
This is actually has a secondary consequence of causing further insulin resistance, especially in skeletal muscle. Which in one sense makes the problem worse. But in another, can help the muscle burn fatty acids if energy expenditure goes up.
An additional consequence of fat cell insulin resistance is that incoming calories no longer has anywhere to “go”. Generally at this point the muscle is full of carbohydrate and fat (Intramuscular triglyceride) and fat cells are full off fat. So incoming nutrients tend to sit in the bloodstream leading to high blood glucose, high blood fatty acids, high blood cholesterol and all of the other hallmarks of Metabolic Syndrome.
On that note, one of the drugs used to treat the Metabolic Syndrome actually increases the number of fat cells someone has. This provides a larger “sink” for incoming calories, at least temporarily lowering blood glucose, etc. But in the long-term it ultimately makes the problem worse as the person now has more fat cells.
Insulin Resistance as an Adaptation
In a very real sense, this is an adaptation to obesity that attempts to push calories away from fat cells (towards burning elsewhere). I’ve talked about in my books (especially The Ultimate Diet 2.0) that, in this sense, under certain conditions, being insulin resistant can be a “good” thing.
Tangentially, insulin resistance appears to have developed as a positive adaptation to low-carbohydrate conditions during our evolution most likely to spare glucose for use by the brain. It’s only under high-carbohydrate intake conditions (i.e. the modern diet) that insulin resistance becomes a bad thing. Keep this in mind when you read articles talking about how low-carbohydrate/ketogenic diets induce insulin resistance. They do but it’s for a good reason.
That is, the insulin resistance that develops is actually a “good thing” and this is true under both low-carbohydrate and low-calorie dieting conditions. If the fat cell are trying to keep calories out (and push them away to be burned off), this can facilitate fat loss.
That insulin resistance is actually a “good thing” is especially true under both low-carbohydrate and low-calorie dieting conditions. If the fat cells are trying to keep calories out (and push them to burning elsewhere), this can facilitate fat loss.
In this vein, one of the major adaptations to getting leaner is a massive increase in insulin sensitivity, which is part of what makes further fat mobilization more difficult as folks get leaner. I’d mention that this is exactly the opposite of how most people think it works. In at least some research, insulin sensitivity actually predicts weight gain, not the other way around.
And this actually makes some sense: the time you’re at the greatest risk for weight/fat regain is at the end of a diet when insulin sensitivity is high. Insulin can now store incoming calorie with great efficiency. Along with the other adaptations to dieting, this facilitates fat gain.
But going back to the obese beginner, this adaptation is only beneficial IF other tissues are able to optimally burn those fatty acids off. Having plenty of fatty acids floating around only helps fat loss if they can be burned for fuel. But I’m getting ahead of myself.
I’ll finish up this section by pointing out that insulin resistance has some practical implications in terms of the choice of diets. Whether or not they have an actual “metabolic advantage” in terms of fat loss (they don’t), it’s become clear that reduced carbohydrate (and increased protein/fat) diets improve a variety of metabolic parameters associated with the metabolic syndrome. This is often true even in the absence of weight or fat loss. But they cause an even more profound effect if weight and fat are lost.
I’ll come back to this topic later in the series. I have also talked about the impact of insulin sensitivity and insulin resistance on fat loss previously.
.
RER, RQ, and NPRQ
No, not the talk-radio station. Let me get a little bit technical and talk about fuel utilization in the body and how it is measured. Depending on what you read, you will often see the acronyms RER, RQ and NPRQ thrown around. Let me explain what they are and what they mean.
First off, RER refers to respiratory exchange ratio, RQ to respiratory quotient and NPRQ to non-protein respiratory quotient. All three refer to essentially the same thing and I’ll use RER from here on out.
And what they refer to is the mix of fuel being used by the body both at rest and during activity. I won’t bore you with the details, basically these three things are all a measure of the ratio of oxygen being consumed and carbon dioxide being produced and this is used as a proxy for fuel use in the body.
That is, biochemically we know that the burning of carbohydrates has an RER of 1.0 (1 molecule of O2 metabolized for each molecule of CO2). The burning of fat has an RER of 0.7. Protein is somewhere in the middle (about 0.86 or so depending on the protein source).
So researchers bring people into the lab, do a bunch of technical stuff that require a bunch of assumptions being met and determine RER. And that gives an indication of what fuel is being used by the body either at rest or during exercise.
Under most conditions, researchers only focus on carbohydrate and fat and ignore protein. That’s what NPRQ actually refers to: the non-protein respiratory quotient. I’ll ignore protein here since it usually makes up such a tiny percentage of total fuel use to begin with.
Here’s a chart of RER values and the percentage carbohydrate or fats that are burned.
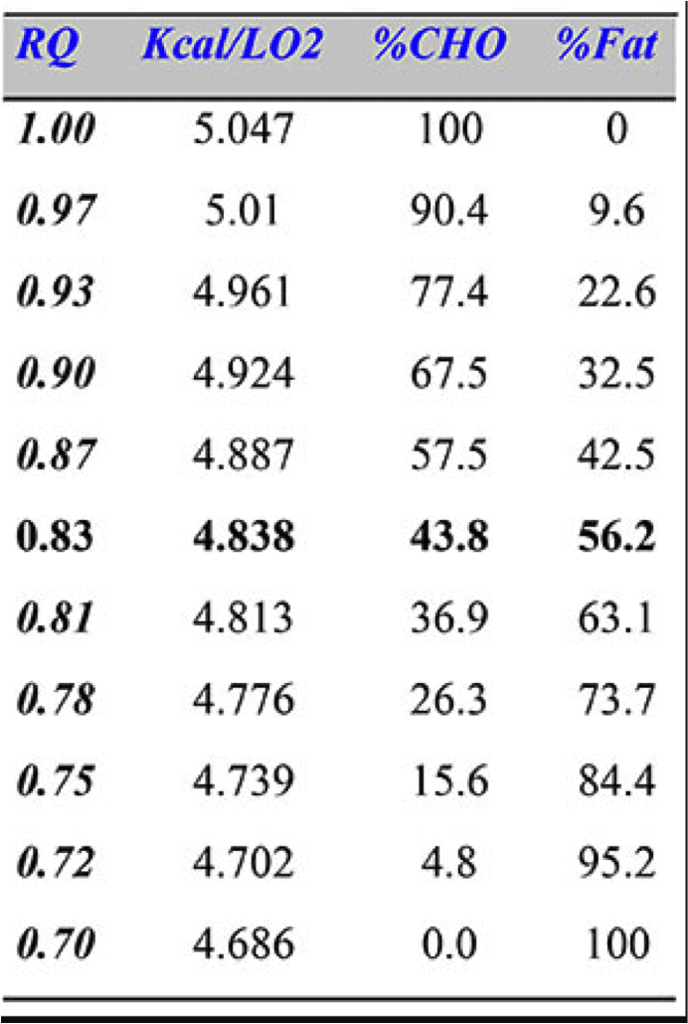
You can see that a value 0f 0.7 is 100% fat use, 1.0 is 100% carb use and everything else is in-between. There are some odd situations where RER may be measured below 0.7 but this is an artifact related to carbox dioxide metabolism under certain conditions. Obviously you can’t burn more than 100% fat.
What Determines RER?
So what determines RER? Well a bunch of things. Gender is one and RER can change throughout the menstrual cycle with women typically burning more carbs in the first half of the cycle and more fat in the second half of the cycle. Training status is another and generally regular training will lower RER, meaning that the body relies more heavily on fat. There is assuredly a genetic component to all of this.
Of some importance, habitual diet can affect things massively, in at least two ways. The first is that the body adjusts nutrient intake, storage and oxidation to habitual intake. Ignoring protein once again, carbohydrate intake tends to have the biggest influence. When you eat more carbohydrates you burn more carbohydrates for fuel while burning less fat (RER goes up). This is actually how eating excessive carbohydrates can lead to fat gain.
In a related vein, the status of muscle glycogen impacts RER profoundly. When the muscle is full of glycogen, it tends to use carbohydrate fo fuel which means it doesn’t burn much fat. When muscle glycogen is depleted, the muscle will shift to using more fat for fuel. I’ll talk about this more when I discuss diet in Part 2.
The Relevance of RER to the Obese Beginner
So what’s my point? Well, two points actually.
The first is that many studies have found that the obese have a higher resting RER on average. That is they tend to preferentially burn carbohydrates for fuel. Combined with a high-fat intake, this leads to fat gain. In a similar vein, resting RER is predictive of RER during activity. People who burn more carbs at rest burn more carbs during exercise. So it’s a double whammy where their bodies are not utilizing fat for fuel very well.
The second is that the habitual diet can impact can be a cause of further problems such as impaired fat burning and a preferential burning of carbohydrates.
Which brings me in a roundabout way to my quote from earlier in this article. The combination of factors I’ve described, the insulin resistance that commonly accompanies obesity along with a high resting RER due to habitual diet and inactivity leads to a situation where there are lots of fatty acids in the bloodstream but the body is bad at using them for fuel. I’ll discuss how to fix this in later parts of the series.
Right now let me talk about the next metabolic “defect”..
Impaired Mitochondrial Function
So as everyone learned in high school biology, mitochondria are the powerhouse of the cell. Specifically in this case they are specialized bits of the cell where things are burned for energy, especially fatty acids. So fatty acids enter the mitochondria undergo a bunch of chemical stuff and energy (ATP) is produced.
Well a number of studies over the years have found that mitochondrial function is impaired in obese individuals. Mind you, not everyone finds this data convincing and others think the problem is actually low oxygen delivery to the skeletal muscle. Which, while interesting technically, doesn’t really change how the problem should be approached. Meaning that I’ll continue referring to the issue as a mitochondrial defect going forwards.
In addition, research has found that the obese don’t show the same ability to switch to fat oxidation during activity. They have lost what is called metabolic flexibility, the ability to switch between fuels as necessary.
A final consequence is that, since fatty acids have nowhere to go, they tend to get stored in inapprpriate places such as the liver or pancreas. This process is called ectopic fat storage and causes damage to those organs and more health issues down the road. But I don’t want to get too deeply into that.
Cause or Effect?
Now a question that always raises its ugly head here is what’s causing what? That is, does impaired mitochondrial function/etc. predispose some individuals to become obese? Or does obesity cause the mitochondria to become dysfunctional somehow?
Tangentially you can replace mitochondria with any metabolic “defect” seen in obesity above. There’s always the big question of which comes first: the defect or the obesity. And this can be difficult to determine sometimes.
What it requires is for researchers to find a group of people, measure some stuff and follow them to see who becomes obese. That lets them determine that some baseline characteristic is part of the predisposition to obesity. Alternately, they can see if those “defects” improve or disappears when people lose fat. If it does, that at least suggests that the “defect” was caused by the development of obesity.
Of course, there is a third possibility which is often forgotten. It’s always possible that some sub-clinical “defect” causes someone to be predisposed towards obesity and becoming obese just makes the problem worse. So perhaps someone is born with low mitochondrial function or a high resting RER and this causes them to start gaining fat which makes things worse which leads to more fat gain which……
To be honest, it’s usually this third situation going on. Someone is starting with some set of biological characteristics that, in the modern environment, predispose them to gain fat and the problems just get worse and worse in a feedback loop.
Now, in most cases, a lot of these “defects” do at least improve when weight/fat loss or an increase in activity. In the case of metabolic syndrome, both tend to improve and reverse most parts of the syndrome.
Note that improve is not the same as eliminate.
I would at least point people to the Biggest Loser Feedback for the improvements he saw in heart rate, blood pressure and blood glucose in a mere 14 days. He got essentially normalization in a miniscule period of time secondary to a massive increase in activity and equally massive weight loss.
In the case of mitochondrial dysfunction/etc. this certainly seems to be the case where the “defect” improves with increased activity. But this is honestly old news. Regular aerobic exercise is known to improve mitochondrial number and function (and blood flow to muscle, for the record). It would be surprising if this didn’t improve with activity unless there were some massive pathophysiology present.
Since this is getting long, I’ll wrap it up here and continue with some other physiological considerations for the obese beginner in Training the Obese Beginner: Part 2
Facebook Comments