Having finished examined the definition of overtraining in Part 3 I want to move into some other topics. Today I will focus on the idea of there being different “types” of overtraining. This will lead into a bit more detailed look of the physiology behind what is occurring in overtraining.
Table of Contents
A-Type and B-Type Overtraining
As I imagine most readers are at least vaguely familiar with, the human nervous system is generally divided into the sympathetic nervous system and parasympathetic nervous system. The sympathetic nervous system handles responses related to stress and fear. Heart rate goes up, blood pressure goes up, etc. In contrast, the parasympathetic doest the opposite, slowing heart rate, blood pressure, etc.
In a very simplistic sense you would want high sympathetic tone when you are training and increased parasympathetic tone for recovery. While I won’t get into it here, Heart Rate Variability are essentially examining the relative “dominance” of the sympathetic versus parasympathetic systems.
In any case, during the early days of overtraining research, a distinction was made between what was called Addisonic (or A-type) and Basedowic (B-type) overtraining. These were meant to draw similarities to, respectively, Addison’s disease (where the body has overactive parasympathetic dominance) and Basedow’s disease (where it has overactive sympathetic dominance).
I alluded to this very briefly in an earlier part of the series when I mentioned that overtraining may be marked by higher heart rates at a given workload which would be an example of B-type overtraining. In the case where the athlete can’t get their heart rate up at all (which may look like they are getting fitter), that would be A-type overtraining.
The essential idea is that, in the case of A-type overtraining, the body has become parasympathetic dominant. That is the parasympathetic branch of the nervous system is sending out too strong of a signal. As one of the consequences of this you often see a lowered resting heart rate, lowered blood pressure and some other stuff. As I mentioned, this can actually look like the athlete is improving their fitness although their performance still usually sucks. This becomes especially apparent when they try to generate a maximum effort and simply can’t do it.
In contrast, with B-type overtraining, the sympathetic nervous system is dominant, leading to increased resting heart rates, raised blood pressure, etc. And this manifests as a higher heart rate during a fixed workload exercise. Resting heart rate was used for absolute years to try to identify the early onset of overtraining. So you’d track morning heart rate and if it was elevated by 5-10 beats above normal, you needed to rest. Not that most athletes will.
Heart rate variability (HRV) can serve some of the same purpose since a shift towards a lower HRV is indicative of greater sympathetic tone. When this occurs, the athlete is overdriving the system and needs more recovery before they start to really fall off the edge.
Different Sports, Different Types of Overtraining
Originally, it was thought that different types of training caused the different types of overtraining. The basic idea was that high-volume training as in endurance sports would cause parasympathetic dominance while high-intensity training as in strength/power type sports would cause sympathetic dominance.
But it doesn’t seem to work out this way. As I’ll talk about later in this series, you tend to see sympathetic dominance in both types of sports when overtraining starts, regardless of the type of sport. A more current idea is that the early stage of training are marked by sympathetic dominance but this eventually switches to parasympathetic dominance if the imbalanced training load continues.
I’d note that this has a clear link to what happens during stress in general. As I talked about in The Women’s Book at length, what happens in chronic stress is that the body is just chronically producing the hormone cortisol. But after too long a period of this, the system reverses itself and you get an adaptive hypocortisolism, thought to be a protective adaptation by the body.
In fact, A-type overtraining was originally conceptualized as occurring due to a failure of the adrenal glands to keep up with the demands of training. Yes, this sounds like the whole concept of adrenal fatigue, except that it isn’t real. Rather it’s an adaptation whereby the system eventually just shuts itself down to protect the body.
More to the point, overtraining can get complicated by the fact that different responses to a long-term excessive imbalance between training recovery are possible. Certainly sympathetic overtraining seems to be the more common form. And it’s likely the earlier form.
But it’s also possible for a parasympathetic type of overtraining to occur, one which looks kind of like a beneficial training response. Resting heart rate is down, heart rate at submaximal work loads is down, etc.
And this can make diagnosing overtraining a problem.
Symptoms of Overtraining
Over the years, researchers and coaches have identified a number of common symptoms that tend to occur with or sometimes prior to true overtraining/underperformance and I want to look at a few of them below. I don’t tend to discuss each in extreme detail. However, at least knowing what some of the symptoms are gives athletes and coaches a rough tool to monitor what’s going on with the athlete. This list is also necessary for other topics I’m going to discuss.
I call it a rough indicator for reasons I’ll detail later. A problem with all of this is that the signs and symptoms of overtraining are never universal. They don’t occur in all situations or even in all athletes. So they certainly aren’t perfect. But most of these are at least common enough to be worth paying attention to. Let me also note that this list isn’t meant to be comprehensive. These are just a few of the most common symptoms that tend to show up in an athlete when overtraining is about to occur or has already occurred.
- Constant muscular fatigue and/or soreness (both muscle and joints).
- Lack of motivation to train/lethargy/overall fatigue.
- Higher incidence of illness.
- Depression in susceptible athletes. Hostility in others.
- Sleep disruptions.
- Impaired appetite.
- Increased resting heart rate and blood pressure (except in the case of B-type overtraining).
As you can sort of see it’s a rather mixed bag of symptoms, and again, that’s only a handful of them. What may stand out to you, and I deliberately sort of randomly ordered them in the list is that some seem to be related solely to muscles and such while others seem to be more brain (or at least centrally) related. Number 4 is a good example as this is a change in mood state. What could that possibly have to do with overtraining?
Central and Peripheral Overtraining
For reasons primarily of practicality and convenience, the body is often divided rather roughly into central (meaning the brain and central nervous system) and peripheral (muscle and peripheral nervous system) systems. While this helps simplify discussions, it’s critical to realize that the systems aren’t separate in the least.
Rather, as I discussed previously in a diet context, the central and peripheral systems are interacting and communicating with one another constantly. The brain talks to the body and the body talks back to the brain. This occurs through the nervous system, hormones, etc.
In the case of eating behaviors and body weight regulation, the gut, fat cells and everything peripheral is sending signals to the brain (about such things as how much you’re eating, energy balance, fuel utilization) and the brain is sending signals back out to the body or adapting to them.
In the case of the body and training, while the brain is sending signals to the muscles about how to contract or what to do, the muscles are sending signals back to the brain (about energy stores, damage and other factors). Discussing the two systems separately and independently is convenient but ultimately wrong.
But in the early days of overtraining research, a distinction was often made between peripheral overtraining and central overtraining. As with A-type and B-type the idea was that each would be impacted to a greater or lesser degree by the type of training done. Certainly there is an element of truth to the idea in that certain types of training tend to stress the nervous system more while others stress the muscles.
In fatigue research a distinction is made between central and peripheral fatigue and this is just the overtraining extension of that. But even here it’s never one or the other, it’s simply an issue of proportion. All types of training stress both muscle and nervous system. It’s just a matter of degrees.
And when you then realize that each system is “talking” to the other in what amounts to a loop, you find that the distinction starts to have less and less meaning. As I said above, the brain talks to the body and the body talks back to the brain.
But early ideas held that you couldn’t “overtrain” so long as you rotated what muscles every day or that you could only overtraining with certain types of training became entrenched in the lore of training. And it was all due to this artificial separation between central and peripheral systems. And it caused people to make some big mistakes.
As one example, Fred Hatfield not only wrote that central overtraining didn’t exist, but that you could train as much and as hard as you wanted so long as you alternated muscle groups. That is, so long as you avoided local overstress of a given set of muscles, you were fine because there was no such thing as central overtraining. Sadly he was completely and utterly wrong as many who tried to follow his ABC system found out the hard way.
Returning to my time in Salt Lake again, the same Russian coach I mentioned believed that it was impossible to overtrain if you weren’t doing training that stressed the cardiovascular system. So long as it was just local muscular work, he felt you were fine no matter how much of it you did. Thea idea had been discredited by the 80’s but this was a man who hadn’t learned anything new since the 1970’s. When one of his athletes started to look overtrained he “knew” it was impossible since they weren’t doing central work. And he was wrong.
Going back to my time in SLC, I saw a fantastic example of this, again with the Russian coach who had buried our team in volume; he believed that it was impossible to overtrain if you weren’t doing training that stressed the cardiovascular system. So long as it was just local muscular work, he felt you were fine. Which is an idea that got discredited by probably the 1980’s or so; sadly he hadn’t learned anything new since the 70’s.
The reality, as one luminary in the field of bodybuilding once put it “Every day is kidney day”. Bu that he meant that all training is a stress to the entire body because all stress is a stress to the entire body. Sure, training arms is a lot less stress than training legs. But you can’t ever separate peripheral and central training completely.
Make no mistake, there is some merit to the idea that peripheral and central fatigue/overtraining have distinct causes or at least manifestations. If you look back up at the list of symptoms, you can see that some are distinctly peripheral (muscle fatigue) and others are distinctly central (sleep, depression).
But you can’t cleanly separate the two in any truly meaningful way. And I’m beating this dead horse to lead into the next topic.
What Causes Overtraining: Redux
Previously I presented the idea that the global “cause” of overtraining was a long-term imbalance between training (and other) stressors and recovery. While this is useful in a practical sense, it doesn’t get to the real root of the matter. That is, what biological/physiological processes are causing the issues that occur in the first place. While these might seem somewhat impractical sin
So what, at the end of the day what “causes” overtraining?
One early thought was that it was due to the depletion of muscle glycogen (carbohydrate stored within the muscle). The idea was that inadequate calorie/carbohdyrate intake coupled with too much training would deplete the body’s stores and that would cause problems. Some studies seemed to bear this out as a hard week of training with insufficient carbohydrate intake can deplete glycogen. And problems were occasionally seen.
But studies that used heavy training with tons of carbohydrates still couldn’t prevent underperformance from occurring. Glycogen depletion wasn’t helping but maintaining glycogen wasn’t sufficient to prevent it. It was at most part of the problem but it wasn’t the whole issue.
Many other things were examined, often focusing on biological markers that indicated (probably more than caused) overtraining. I already mentioned that testosterone/cortisol ratio where a reduction in testosterone and an increase in cortisol often accompanied overtraining. There were others but they all seemed to really be a marker that overtraining was occurring and the body wasn’t keeping up with the stress load but they weren’t the cause.
This was further complicated by the fact that some of the factors being examined were neurochemical in nature, changes in brain chemistry. And studies using the Profile of Mood Score (POMS) had shown a distinct change in scores with overtraining. Along with the other observations of central changes (i.e. mood, sleep, a lack of enthusiasm), nobody could really put together a good model to tie them all together.
And then someone did.
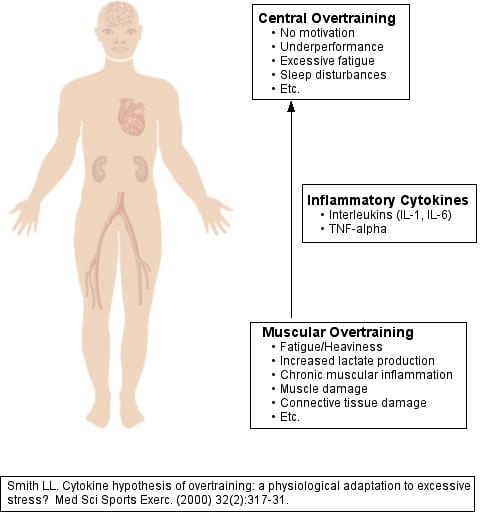
The Cytokine Hypothesis of Overtraining
One of the earliest models of overtraining that tied muscular to central factors was presented in a paper titled Cytokine hypothesis of overtraining: a physiological adaptation to excessive stress? by LL Smith. He’s written several others in a similar vein. I’ll come back to a more recent paper in a little bit.
In it he examined all of the different data points that had been developed over the years and built up a model of overtraining that seemed to tie everything together. It probably wasn’t the entire picture at the time but it was one of the best earliest models I had seen.
For background, cytokines are small, fairly short-lived chemical messengers that do all kinds of things in the body. A singular example I’ll focus on is IL-6 or Interleukin-6. Released from both skeletal muscle and fat cells, IL-6 does a number of interesting things. Acutely, one is to increase fat mobilization and oxidation and in this vein IL-6 is released in response to glycogen depletion in the muscle. Chronically however, it causes inflammation.
IL-6 can also cause fatigue during exercise. And here’s the key thing: it does this by altering neurochemistry in the brain in such a way as to cause fatigue centrally. So if you take someone who is well-rested and inject IL-6 into them, their exercise performance goes down and they will report fatigue and lethargy.
So when muscle starts pumping out IL-6 into the system chronically it goes to the brain and makes people fatigue sooner. This happens when glycogen levels get depleted and we know that exercise performance is harmed when this occurs. And suddenly we have a potential link from the earlier observation of muscle glycogen being involved in overtraining.
One last thing, elevated IL-6 levels seem to be involved in depression. Which I mentioned was one of the common symptoms of overtraining. Now we’er onto something.
Of course there are dozens of cytokines being released from all over the body (and now they are more likely to be called myokines if they come from muscle, hepatokines if they come from liver, etc) and they are assuredly all interacting in horrifically complex ways that it will take researchers years to work out. But that’s good, it keeps the scientists off the streets and out of scientist gangs. But cytokines and how they suddenly give us a way to link the peripheral system (muscle, fat, liver) to the central system in terms of communication.
An easy to understand example is the flu which most have gotten at least once. When you get it, your whole body aches including your muscles and joints. You lose your appetite. You may get depressed. And you want to sleep all the time. Basically the immune system in on part of the body causes this big cytokine response that goes to the brain and makes you feel crappy so that you’ll rest and get over being sick. That is, the peripheral response generates an additional central manifestation. You don’t just get achy joints and muscles but your behavior changes so that you’ll rest.
The body is pretty smart sometimes. Unfortunately, people are sometimes not so smart. Because while we’ll all pretty much rest and sleep when we have the flu, insane athletes will frequently keep hammering themselves with too much volume and intensity in the face of this mounting fatigue and lethargy. Their bodies are telling them to rest and they are ignoring it. If they were sick, they’d rest. Faced with underperformance, they often train harder. And they just keep digging the whole deeper.
And this model would seem to be a pretty way to link all of the disparate symptoms of overtraining. Basically Smith argued that chronic underrecovery to training causes muscles and joints to become chronically inflamed, pumping out cytokines like IL-6 that cause systemic inflammation. Studies at the time had found an increase in various inflammatory cytokines in overtrained athletes.
Not only did this make the muscles and joints achy, along with wonking the immune system, these compound would change neurochemistry and make the athlete lethargic, lose motivation, become depressed (or sometimes hostile), lose their appetite and have sleep problems. Those changes in central factors would then impair exercise performance on top of everything else that was going on.
Peripheral problems were directly causing central issues as I’ve shown graphically here.
So in this model, overtraining essentially was your body telling you to knock it off, rest and recover by making you feel like crap. Just like when you have the flu. But, as I said, while people will rest when they are sick, obsessive athletes often won’t rest when they are performing badly. They simply ignore those feedback signals and fight through them.
And this creates another loop whereby underperformance from excessive training/underrecovery leads to more excessive training and worse recovery which drives more training and worse recovery until the athlete finally crashes.
And as it turns out, while Smith came up with his hypothesis quite some time ago he seems to have gotten it basically right. A recent paper titled Intramuscular Mechanisms of Overtraining examined all of the research in terms of the muscular causes of overtraining. They examined, glycogen depletion, muscle damage, inflammation and reactive oxygen species (ROS, free radicals) concluding:
Current data implicates reactive oxygen and nitrogen species (ROS) and inflammatory pathways as the most likely mechanisms contributing to OTS in skeletal muscle. Finally, we allude to potential interventions that can mitigate OTS in skeletal muscle.
So for all practical purposes, Smith got it right enough. Those peripheral muscular factors are sending signals to the brain causing a host of behavioral changes to occur. And that model really wrapped up all of those disparate symptoms into a nice little package. This was on top of truly making the point that any division of central and peripheral overtraining is utterly meaningless.
It’s a shockingly simple and neat model but certainly seems to explain most of what’s been observed over decades of study on the topic.
And with that background, let me look next at some of the tactics that athletes can use to try to prevent overtraining from occurring in the first place.
Read A Guide to Overtraining and Overreaching: Part 5.
Similar Posts:
- Overtraining and Overreaching: Part 6
- Overtraining and Overreaching: Part 2
- The Importance of Rest
- Overtraining and Overreaching: Part 5
- Endurance Training Method 4: Interval Training Part 2
Lyle,
With that Russian coach you mentioned, how does a guy like that even end up being allowed to work with athletes here? Were the higher ups so impressed by his apparent success back in the Motherland (any success likely being the sole product of the numbers game you mentioned) that they ignored what he was doing once he got here?
I also wanted to ask your take on handling a situation where an athlete may not be suffering from true overtraining syndrome but in which the drive isn’t there, psychological doldrums/burnout having set in. In this type of special case, do you feel that some degree of a full break may be required, to see if it refreshes the athlete and brings back that focus and drive. Or would you try to let the athlete work through that and possibly just pull back a bit.
Any detraining, while undesirable, seems like it would be less of a big deal in such a case, since true burnout would signal the end for an athlete………..or at the very least a significantly extended period away as he “searches” for the spark that’s gone missing.
There are no requirements to be a ‘coach’ in the United States. If you say you’re a coach, you’re a coach and you basically need a whistle and a stopwatch and you’re good to go. The problem is when the athletes can’t see through their crap to see that they are incompetent.
Your other questions will be answered in Part 6. I’ll only say now as a teaser that the psychological issue of loss of motivation is often the first early symptom that shows up before the crash hits. You’ll learn why soon.
Hi Lyle,
Im sorry to burden you with my inquiry as I imagine everyone wants your expertise applied to them specifically. But wanted to know if you think this could be over-training and what is the remedy. Well I’m 35 and have awful genetics. Everyone in my family is obese and I’m terrified of heading down that road so I’m addicted to the gym. I’ve been training since I was 16 and have never been able to quite get it all together. Never had a 6 pack or much definition. I have gained weight going from 165 in high school to 225 15% bf now but it seems that the muscle fat ration has remained the same. I have tried every dietand type of training(high carb, low carb German volume training, negative training, HIIT etc. etc) Right now I’m on the Ketogenic diet for 4 weeks. I have lost weight about 8 lbs. but it seems that I have equally lost just as much muscle. I followed everything you have said to a T in your book. I’m so frustrated. I apply your principles to many clients that I train and they have amazing transformations. My body is so fickle. One day I can see my biceps beginning to split and then the very next day I have no definition at all. I know there are so many variables. But I wonder if I could be over-training. I never cheat on my diet and log my workouts. Over the last year I have mad little to no strength gains. I’m so depressed and frustrated. I hate how my body adapts so quickly. Like I’m programmed for fattness. Please help me.
Right now 70% fat 30% protein 2500 calories. Train whole body M/T Wed/Thur cardio Sat morning glucose depletion work out. Carb up. Sunday cardio back to KEto.
– One unhappy Trainer
Lyle,
Thank you for this. It’s absolutely the best series of articles I’ve found on this topic. I’ve been ‘unable’ (or unwilling) to train for almost a month now due to underrecovery and it doesn’t look like I’ll be feeling well enough to go back to the weight room or even go for a run any time soon. I had spent 2 years training hard while going through a very traumatic divorce from an alcoholic,finishing a postgraduate degree, working full time, caring for my daughter and my two terminally ill parents and was too bull-headed to slow down.
Finally crashed last month when preparing for my first figure contest having changed my training to 5am to fit it in & sticking rigidly to a ketogenic diet given to me by a nutritionist I’d consulted because I felt so awful.I switched gyms to a commercial one around the corner from my work, but started skipping warm ups so I could get to a rack as I knew it’d take me an age to complete the programme as I was so tired. I couldn’t sleep, my mind was constantly racing, I was very, very sore, my lifts dropped back to the level they were at 18 months ago, I was obsessing about tiny details and I was a total, miserable pain to be around inside and outside of the gym.
It’s true that the training wasn’t the issue- the volume and intensity were what I needed to reach my goals and should have been well within my capabilities, but frankly I was the victim of my own ignorance and my ego.Deloading? Foam rolling? More than a handful of starchy vegetables 3 times a week? Not me. My recovery was the one thing that I should have prioritised but I liked to think I was tough enough to train through anything.
I’m now just adapting to eating everything in sight for a while to get over my carb phobia and taking lots of magnesium as well as I-Thenine which ,despite my cynicism, really helps with sleep and trying some eleutherococcus senticosus and ashwagandha (can’t do any harm). It’s been heartening to read this series- I’ve had real issues explaining this to people I train with but honestly, I’ll never let this happen to me again.